The health effects of very-low-calorie diets (VLCDs) adopted for short periods of time (e.g., 5 days) have been the target of much recent in the past. Consuming 400-600 kcal/day would be considered VLCDing. VLCDing for significantly longer periods of time than 5 days can be dangerous, and in some cases potentially fatal. Nevertheless, there is speculation that it can also cure type II diabetes (
).
Intermittent VLCDs mimic in part what probably happened with our ancestors in our evolutionary past. Successful hunting and gathering would lead to weight-maintenance food intake most of the time, with occasional periods of severe food scarcity. This has probably been a regular pattern in our evolutionary history, leading to health-promoting adaptations that are triggered by VLCDs.
The part that VLCDs alone do not mimic is the “hunting and gathering part”, or the exercise required to obtain food when it is scarce. This is an important point, because VLCDs are likely to induce lean body mass loss without exercise, together with body fat loss. VLCDs without exercise are not very natural, even though they can have very positive effects on one’s health, as we’ll see below.
An interesting and well cited study of the effects of VLCDs in participants with type II diabetes was published in 1998 in an article authored by Katherine V. Williams and colleagues (
). The study included 54 participants, and lasted 20 weeks in total. The site of the study was the University of Pittsburgh School of Medicine. The participants were split in three groups, referred to as:
- Standard behavioral therapy (SBT). The participants received a 1,500−1,800 kcal/day diet throughout, with the goal of inducing gradual weight loss.
- Intermittent 1 day/week VLCD (one-day). The participants received a VLCD for 5 consecutive days during week 2, followed by an intermittent VLCD therapy for 1 day/week for 15 weeks, with a 1,500−1,800 kcal/day diet at other times.
- Intermittent 5 day/week VLCD (five-day). The participants received a VLCD for 5 consecutive days during week 2, followed by an intermittent VLCD therapy for 5 consecutive days every 5 weeks (5-day), with a 1,500−1,800 kcal/day diet at other times.
There is a reason behind this complicated arrangement. The researchers wanted to make sure that the average caloric intake for the two VLCD groups was identical, but 18,000-28,000 kcal lower than for the SBT group. The SBT group served as a baseline group.
All of the three diets were designed to make the participants lose weight. Exercise was not manipulated as part of the experiment. The one-day and five-day groups consumed 400-600 kcal/day while VLCDing, with the majority of the calories coming from high-protein-low-fat minimally processed food items – notably lean meat, fish, and fowl.
The graphs below show results in terms of weight loss and fasting plasma glucose (FPG) reduction. They suggest that, while there were significant differences in weight loss between the VLCD groups and the SBT group, the differences in FPG reduction were relatively minor across the three groups.
Glucose was measured in mmol/l and weight in kg. One mmol/l is equivalent to approximately 18 mg/dl (
), and one kg is equivalent to about 2.2 lbs.
The graph below, however, shows a different picture. It shows results in terms of the percentages of participants with HbA1c below 6 percent. The HbA1c is a measure of average blood glucose over a period of a few months (
).
The graph above tells us that the intermittent VLCD interventions, particularly the second (five-day), were reasonably successful at promoting average blood glucose control. A threshold normally used to characterize poor blood glucose control is 7.3 percent (
), which is based on studies of HbA1c levels associated with diabetes complications.
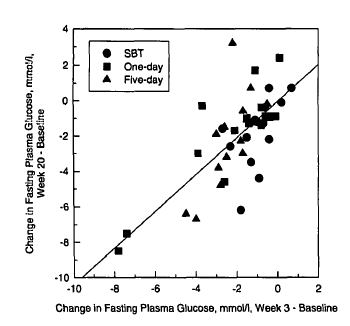
The graph below, which is probably the most telling of all, shows long-term FPG changes (at the 20-week mark) plotted against short-term changes (at the 3-week mark). What this graph tells us is that those who experienced the most improvement right away were the ones with the most improvement in the long term.
This study tells us a few interesting things. Firstly, intermittent VLCDing with a focus on high-protein foods (lean meats) seems to be a powerful way of controlling average blood glucose levels in diabetics. It is essentially a low carbohydrate diet that is also low in calories (
). Secondly, results with respect to FPG levels are not as telling as those in terms of HbA1c levels, even though HbA1c and FPG are highly correlated.
Thirdly, intermittent VLCDing may not actually “cure” diabetes when significant beta cell damage has already occurred (
). This conclusion is speculative, but it follows from the short-term versus long-term results.
It seems that intermittent VLCDing helps diabetics in general with glucose control, but is truly curative for those in which enough beta cell function has been preserved. At least this is one explanation for the fact that those with immediate positive results (at the 3-week mark) tend to be the ones who retain those results over the long term.
The immediate positive results may well be due to those individuals not having reached the point at which significant and irreversible beta cell damage occurred. In other words, this study suggests that intermittent VLCDing can be particularly helpful in the long term for prediabetics.
This third, and speculative, conclusion may have to be revisited in light of the excellent discussion by Roy Taylor on the etiology and reversibility of type II diabetes (
), linked by Evelyn (see comments under this post). This refers to the effects of an extended and more extreme version of VLCD than discussed here, where uninterrupted VLCD would last as long as 8 weeks.
For those who are not diabetic, I personally think it would be better to alternate VLCD with glycogen depleting exercise (e.g., sprints, weight training), every other day or so, with a lot more food consumed on exercise days (
). After excess body fat is lost, it would be advisable to stick to weight-maintenance calorie intake, averaged over a week.